Occipital Neuralgia vs Cervicogenic Headache: Key Differences and Treatment Options

- posted: Oct. 20, 2025
Chronic headaches affect millions of people worldwide, yet distinguishing between different headache disorders remains one of the most challenging aspects of modern pain management. When patients present with neck pain and occipital discomfort, determining whether they have occipital neuralgia vs cervicogenic headache can dramatically impact treatment success and long-term outcomes.
Both conditions frequently present with overlapping symptoms, leading to delayed diagnosis and suboptimal treatment approaches. Understanding the fundamental differences between these two distinct headache disorders is crucial for healthcare providers, patients, and anyone seeking effective pain relief for persistent head and neck pain.
This comprehensive guide explores the key differences between occipital neuralgia and cervicogenic headache, providing essential insights into their clinical features, diagnostic approaches, and evidence-based treatment options. By the end of this article, you’ll have a clear understanding of how to differentiate these conditions and which therapeutic interventions offer the best prospects for finding relief.
Understanding the Key Differences
The distinction between occipital neuralgia and cervicogenic headache lies primarily in their underlying mechanisms and pain characteristics. Occipital neuralgia causes paroxysmal, sharp, stabbing pain in greater, lesser, and third occipital nerve distributions lasting seconds to minutes. This neuropathic condition typically presents as electric shock-like sensations that follow specific anatomical nerve pathways.
In contrast, cervicogenic headache produces dull, tightening, usually unilateral pain originating from cervical spine disorders. This nociceptive referred pain stems from dysfunction in the upper cervical spine and associated musculature, creating a distinctly different pain experience from the sharp, neuralgic pain of occipital neuralgia.

Both conditions share pain pathways through C1, C2, C3 spinal nerves and the trigeminocervical complex, which explains why they can present with similar referred pain patterns. However, their pain locations differ significantly: occipital neuralgia follows specific nerve distributions while cervicogenic headache radiates from neck to frontal-temporal regions.
The fundamental difference lies in pain classification - occipital neuralgia represents neuropathic pain resulting from nerve irritation or damage, while cervicogenic headache is nociceptive referred pain originating from cervical spine structures. This distinction has profound implications for treatment selection and expected outcomes.
Clinical Features and Symptoms
Occipital Neuralgia Characteristics
Occipital neuralgia presents with distinctive clinical features that help differentiate it from other headache disorders. Patients experience sharp, electric shock-like pain in occipital nerve distributions, often described as intense pain that feels like lightning bolts or stabbing sensations. The pain typically follows the anatomical course of the greater occipital nerve, lesser occipital nerve, or third occipital nerve.
The condition may present with unilateral or bilateral involvement, though unilateral presentation is more common. Patients often report paroxysmal episodes lasting a few seconds to several minutes, followed by periods of relative comfort. Between episodes, patients may experience persistent pain or hypersensitivity in the affected areas.
Physical examination reveals positive Tinel sign and tenderness along occipital nerves on palpation. Common causes include whiplash injury, vascular compression, myofascial entrapment, and chronic muscle tension in the upper neck region. Many patients develop allodynia, hyperesthesia, and dysesthesia in affected areas, making even light touch uncomfortable.
Poor posture, particularly forward head posture common in modern work environments, can contribute to occipital nerve irritation and subsequent neuralgia. The condition may be associated with cervical spondylosis or other degenerative changes in the cervical spine.
Cervicogenic Headache Features
Cervicogenic headaches present with distinctly different characteristics compared to occipital neuralgia. Patients experience dull, non-pulsating pain starting in the neck and occipital area, which then spreads to oculofrontal-temporal regions. The pain is typically unilateral and maintains a consistent, steady quality rather than the paroxysmal nature of neuralgic pain.
A hallmark feature of cervicogenic headaches is associated neck pain and limited cervical range of motion. Patients often report stiffness and discomfort in the upper neck region, particularly around the cervical facet joints. The pain is characteristically triggered or worsened by neck movements or specific head positions.
The headache originates from cervical facet joints, intervertebral discs, muscles, and upper cervical structures. Dysfunction in these areas creates referred pain patterns that can mimic other primary headache disorders. Unlike tension headaches or migraines, cervicogenic headaches consistently demonstrate a clear relationship between neck movement and headache symptoms.
Patients may also experience arm pain or radiating discomfort down the shoulder and upper extremity, particularly when nerve root involvement is present. The condition often develops following neck trauma, prolonged poor posture, or degenerative cervical spine changes.
Anatomical Considerations
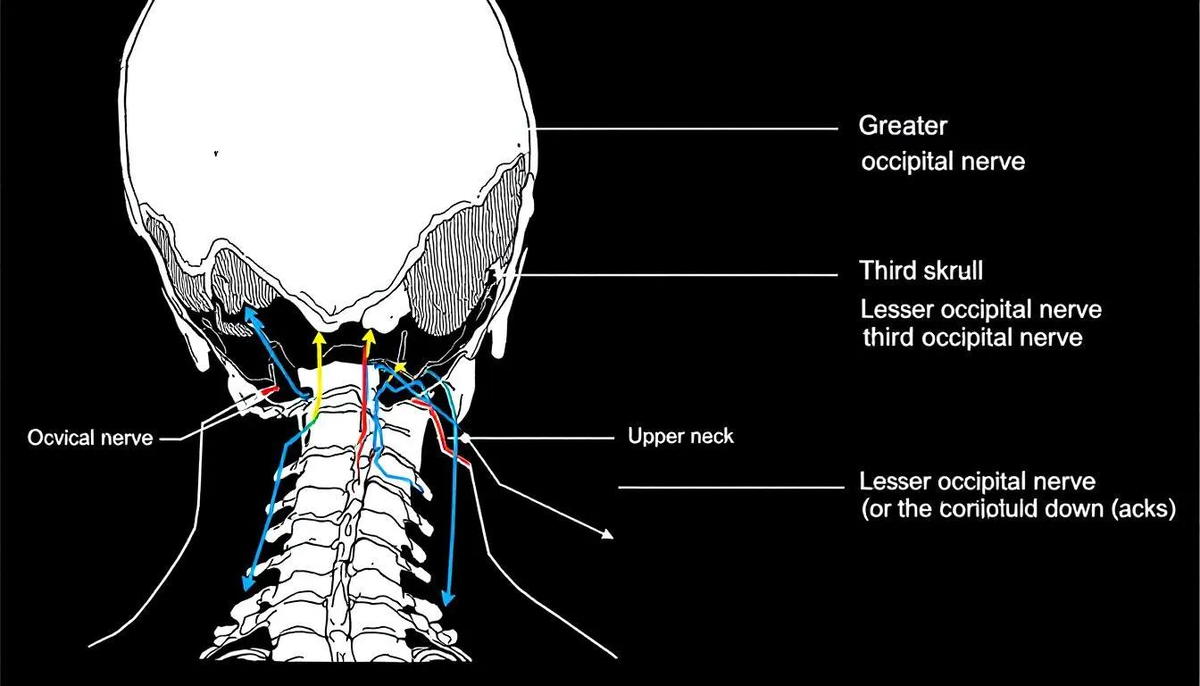
Understanding the anatomical basis of both conditions is essential for accurate diagnosis and effective treatment. The greater occipital nerve arises from the C2 dorsal ramus and innervates the posterior scalp, traveling through the semispinalis capitis muscle and piercing the tendinous insertions at the superior nuchal line before innervating the scalp.
The lesser occipital nerve originates from the C2-C3 ventral rami within the cervical plexus, providing sensory innervation to the lateral occipital region and posterior auricular area. The third occipital nerve, arising from the C3 dorsal ramus, provides sensation to the C2-C3 facet joint and contributes to upper neck proprioception.
The trigeminocervical complex represents a crucial anatomical structure that integrates sensory input from both cervical and trigeminal nerves. This convergence mechanism explains why dysfunction in the upper cervical spine can produce referred pain in trigeminal nerve distribution areas, including the forehead, temples, and orbital regions.
Shared neural pathways between the upper cervical nerves and trigeminal system explain the similar referral patterns seen in both conditions. The nervous system processes nociceptive input from cervical structures and occipital nerves through overlapping pathways, contributing to the diagnostic complexity of these headache disorders.
The cervical facet joints, particularly at the C1-C2 and C2-C3 levels, are richly innervated and serve as common sources of cervicogenic headache. These spinal joints can develop dysfunction due to trauma, degeneration, or biomechanical stress, leading to persistent pain and headache symptoms.
Diagnostic Approach
Clinical History Assessment
Accurate diagnosis begins with a comprehensive clinical history that evaluates pain onset, duration, frequency, location, and triggering factors. Healthcare providers should assess symptoms against the International Headache Society diagnostic criteria for cervicogenic headache, which provide standardized guidelines for diagnosis.
Documentation of response to previous treatments and medication history provides valuable diagnostic clues. Patients with occipital neuralgia often report limited benefit from traditional headache medications, while those with cervicogenic headaches may respond partially to anti-inflammatory treatments or muscle relaxants.
The differential diagnosis must carefully distinguish these conditions from migraine headaches by noting the absence of characteristic migraine features such as nausea, photophobia, phonophobia, and aura. Unlike migraines and cluster headaches, both occipital neuralgia and cervicogenic headaches typically lack autonomic symptoms such as nasal congestion or lacrimation.
Headache episodes should be characterized in terms of frequency, duration, and relationship to neck movements or postures. Patients should be asked about specific triggers, including stress, sleep patterns, and occupational factors that may contribute to chronic neck pain or muscle tension.
Physical Examination
A systematic physical examination is crucial for accurate diagnosis and treatment planning. Testing cervical range of motion, including flexion, extension, lateral flexion, and rotation, helps identify movement restrictions and pain provocation patterns characteristic of cervicogenic headaches.
Palpation of cervical facet joints helps identify the specific spinal levels involved in pain generation. Tenderness over the C1-C2 or C2-C3 facet joints, combined with reproduction of familiar headache symptoms, strongly suggests cervicogenic headache rather than occipital neuralgia.
Examination should include careful palpation along the greater occipital nerve, lesser occipital nerve, and third occipital nerve pathways. Tenderness, hypersensitivity, or reproduction of shooting pain along these nerve distributions supports a diagnosis of occipital neuralgia.

Provocative maneuvers, including controlled movements and pressure application, help reproduce symptoms and identify specific pain generators. The physical exam should also assess for signs of nerve dysfunction, muscle weakness, or other neurological abnormalities that might suggest alternative diagnoses.
Diagnostic Testing
Diagnostic anesthetic blocks of occipital nerves provide both therapeutic and diagnostic value in differentiating these conditions. Greater occipital nerve block and lesser occipital nerve blocks can provide definitive diagnostic information when they result in significant pain relief.
Third occipital nerve blocks help differentiate cervicogenic headache from other headache types by targeting the specific nerve that innervates the C2-C3 facet joint. Positive response to these blocks strongly supports a cervicogenic headache diagnosis.
Advanced imaging studies, including MRI and CT scans, may reveal cervical spine degeneration, disc pathology, or other structural abnormalities contributing to headache symptoms. However, imaging findings must be correlated with clinical presentation, as many asymptomatic individuals show degenerative changes.
Ultrasound evaluation can detect occipital nerve entrapment by measuring nerve cross-sectional area and identifying anatomical variants that may predispose to nerve compression. This non-invasive diagnostic tool is increasingly used to guide treatment decisions and procedural planning.
Differential Diagnosis
Excluding organic causes represents a critical first step in evaluating patients with occipital pain and headache symptoms. Serious underlying conditions such as tumors, fractures, cervical spondylosis with cord compression, and Arnold-Chiari malformation must be ruled out through appropriate imaging and clinical assessment.
The differential diagnosis must consider other common headaches including migraine without aura, tension type headache, and cluster headaches. Each of these conditions has distinct clinical features that help differentiate them from occipital neuralgia and cervicogenic headaches.
Medication overuse headache should be considered in patients with chronic headaches who frequently use pain medications. This condition can complicate the clinical picture and may coexist with either occipital neuralgia or cervicogenic headache, requiring specific treatment approaches.
Postherpetic neuralgia affecting the occipital region can mimic occipital neuralgia but typically has a clear history of herpes zoster infection. Other neuralgic conditions such as trigeminal neuralgia may present with similar sharp, shooting pain but follow different anatomical distributions.
Both occipital neuralgia and cervicogenic headaches can coexist with other headache disorders, including migraine and cervicogenic headaches occurring in the same patient. This overlap requires individual assessment and treatment of each condition to achieve optimal outcomes.
Treatment Options
Conservative Management
Pain education and self-care strategies form the foundation of conservative treatment for both conditions. Patients benefit from understanding their diagnosis, learning about contributing factors, and developing coping strategies for managing chronic headaches and persistent pain.
Physical therapy plays a crucial role in treating both conditions, focusing on reducing muscle tension, improving posture, and restoring normal cervical spine mechanics. Therapeutic exercises targeting the upper cervical spine can significantly improve range of motion and reduce headache frequency.

Pharmacological management includes NSAIDs for anti-inflammatory effects, tricyclic antidepressants for neuropathic pain, muscle relaxants for associated muscle tension, and anticonvulsants for neuropathic pain components. The choice of medication should be individualized based on pain characteristics and patient factors.
Transcutaneous electrical nerve stimulation (TENS) therapy provides non-invasive pain relief for both occipital neuralgia and cervicogenic headache. This complementary and integrative health approach can be particularly helpful for patients seeking drug-free treatment options.
Interventional Treatments for Occipital Neuralgia
Greater occipital nerve block and lesser occipital nerve blocks represent first-line interventional treatments, providing weeks to months of pain relief in many patients. These procedures can be repeated as needed and often provide both diagnostic and therapeutic benefits.
Pulsed radiofrequency treatment of the occipital nerves offers longer-lasting relief, with studies showing 50-70% pain relief lasting 3-7.5 months in appropriately selected patients. This radiofrequency treatment provides neuromodulation without causing permanent nerve damage.
Botulinum toxin injections have shown efficacy for neuropathic-type sharp pain associated with occipital neuralgia. This treatment option is particularly useful for patients who experience both neuralgic pain and associated muscle tension in the occipital region.
Occipital nerve stimulation represents an advanced treatment option for refractory cases, with studies demonstrating greater than 50% pain relief in carefully selected patients. This neuromodulation technique requires surgical implantation but can provide significant long-term benefits.
Interventional Treatments for Cervicogenic Headache
Cervical medial branch block followed by radiofrequency ablation of the cervical facet joints provides longer-term relief for cervicogenic headaches originating from facet joint dysfunction. This approach targets the specific pain generators in the cervical spine.
Third occipital nerve pulsed radiofrequency specifically targets the nerve innervating the C2-C3 facet joint, which is commonly involved in cervicogenic headache. This targeted approach can provide months of relief with minimal risk of complications.
Deep cervical plexus blocks and epidural corticosteroid injections may be appropriate for patients with cervicogenic headaches associated with disc pathology or nerve root irritation. These interventions address inflammation and provide pain relief.
A combined approach targeting both occipital nerves and cervical structures may be necessary for patients with overlapping symptoms or multiple pain generators. This comprehensive strategy addresses all potential sources of head and neck pain.
Procedural Techniques
Occipital Nerve Injection Technique
The landmark-based approach for greater occipital nerve block targets the medial third of the line between the external occipital protuberance and mastoid process. This technique relies on palpable anatomical landmarks and has high success rates when performed correctly.
Ultrasound guidance at the C2 level provides an alternative targeting method that allows direct visualization of the nerve and surrounding structures. This advanced technique may improve accuracy and reduce the risk of complications, particularly in patients with variant anatomy.

Lesser occipital nerve blocks are performed approximately 4-6 cm below the occipital protuberance, 6-7 cm lateral from the midline. This nerve is more superficial and easier to target than the greater occipital nerve, making it an excellent starting point for diagnosis.
Proper needle placement and injection technique are crucial for successful outcomes. The injection should be performed slowly with frequent aspiration to avoid intravascular injection, and the total volume should be limited to prevent excessive tissue distension.
Pulsed Radiofrequency Protocol
Electrical stimulation at 50Hz confirms proper needle proximity to the target nerve before radiofrequency treatment begins. This confirmation step ensures accurate targeting and reduces the risk of incomplete treatment or complications.
Pulsed radiofrequency is applied at 45V with 20ms pulses at 2Hz frequency for 2-4 minutes, maintaining tissue temperature at a maximum of 42°C. This protocol provides neuromodulation without causing thermal nerve destruction.
Multiple treatment cycles may improve outcomes, with some practitioners performing 2-3 cycles during a single session. The pulsed nature of the treatment allows tissue cooling between pulses, preventing thermal damage while achieving therapeutic effects.
Post-procedure monitoring includes assessment of sensory function and immediate pain relief. Patients should be educated about expected outcomes and potential temporary increase in pain before improvement occurs.
Complications and Risks
Minor complications from pulsed radiofrequency include temporary worsening of pain in approximately 10-15% of patients, typically resolving within 1-2 weeks. This transient increase in discomfort should be differentiated from treatment failure or serious complications.
Repeated occipital nerve injections carry the risk of skin atrophy and hair loss from corticosteroid use, particularly with frequent treatments or high steroid doses. Patients should be counseled about these cosmetic risks before treatment.
Surgical interventions for refractory cases carry inherent risks including infection, bleeding, neuroma formation, and the development of anesthesia dolorosa. These serious complications underscore the importance of conservative management before considering surgical options.
Occipital nerve stimulation complications include lead migration in 18-26% of patients, infection in 4.7-14%, and skin erosion in 5.6% of cases. While these rates may seem concerning, they compare favorably to other implantable neurostimulation devices when performed by experienced teams.
Rare but serious complications can include intravascular injection leading to systemic toxicity, infection at injection sites, and allergic reactions to local anesthetics or corticosteroids. Proper technique and sterile procedures minimize these risks significantly.
Prognosis and Long-term Management
Treatment outcomes for occipital neuralgia favor pulsed radiofrequency of occipital nerves over conventional radiofrequency or other interventional treatments. Studies consistently show superior pain relief and longer duration of benefit with pulsed radiofrequency techniques.
Cervicogenic headache responds well to radiofrequency treatment of cervical facet joints, particularly when combined with physical medicine approaches addressing muscle dysfunction and biomechanical factors. The combination of interventional treatments and rehabilitation yields the best long-term outcomes.
Both conditions may require a multimodal approach combining conservative treatments, interventional procedures, and lifestyle modifications. This comprehensive strategy addresses multiple aspects of the pain experience and maximizes the chances of sustained improvement.
Early diagnosis and appropriate treatment significantly improve long-term outcomes for both conditions. Delays in diagnosis or inappropriate treatment can lead to central sensitization and more difficult-to-treat chronic pain syndromes.
Regular follow-up assessment is necessary to adjust treatment plans, monitor for treatment effects, and identify any changes in symptoms that might suggest disease progression or the development of additional pain generators. The treatment plan should evolve based on patient response and changing clinical circumstances.
Patients with multiple sclerosis or other neurological conditions may have modified prognoses and require specialized management approaches. These comorbidities can complicate both diagnosis and treatment, necessitating coordination with neurological specialists.
Conclusion
Occipital neuralgia and cervicogenic headache represent distinct secondary headache disorders with overlapping symptoms that can challenge even experienced clinicians. Understanding their fundamental differences in pain characteristics, anatomical origins, and response to treatment is essential for providing effective care.
Accurate diagnosis relies on careful clinical history taking, systematic physical examination, and judicious use of diagnostic nerve blocks. The distinction between neuropathic pain in occipital neuralgia and nociceptive referred pain in cervicogenic headache guides treatment selection and prognostic expectations.
Treatment approaches differ significantly between these conditions: occipital neuralgia benefits most from nerve-targeted therapies including occipital nerve blocks and pulsed radiofrequency, while cervicogenic headache responds best to cervical spine interventions such as facet joint treatments and physical therapy.
Both conditions share nociceptive pathways through the trigeminocervical complex, explaining their similar pain referral patterns and the diagnostic challenges they present. This shared anatomy also explains why some patients may benefit from combined treatment approaches targeting multiple pain generators.
The evidence-based guidelines and curr pain headache rep literature consistently support a multidisciplinary approach using conservative, interventional, and when necessary, surgical options to provide optimal patient outcomes. Success depends on accurate diagnosis, appropriate treatment selection, and ongoing management tailored to individual patient needs.
For patients struggling with chronic headaches and neck pain, seeking evaluation from specialists familiar with these conditions can make the difference between continued suffering and finding relief. Early intervention and proper diagnosis remain the keys to successful long-term management of both occipital neuralgia and cervicogenic headache.


